
Dive Brief:
-
Medicare Advantage enrollees with chronic conditions had 23% fewer inpatient stays and 33% fewer emergency room visits than beneficiaries in traditional fee-for-service Medicare, according to an Avalere Health study released Wednesday. There were similar results for dual-eligible beneficiaries, among which MA recipients had 33% fewer hospitalizations, 42% fewer ER visits and 20% lower costs.
-
Chronic care patients with MA plans also performed better than those in FFS in higher rates of preventive screenings and tests, along with other key quality measures. Among clinically complex and dual-eligible/low-income subsidy beneficiaries, cost savings and quality of health were significantly better for MA beneficiaries than FFS.
-
The study sampled more than 1 million beneficiaries in MA and FFS each and compared metrics in three populations with chronic conditions: hypertension, hyperlipidemia and diabetes — all of which are in the top five most common conditions among Medicare recipients.
Dive Insight:
Evidence continues to mount on the relative success of MA compared to FFS, and the program remains popular with payers due to the stability of its marketplace. It's also popular among patients. People usually don’t switch back from MA plans after leaving traditional Medicare.
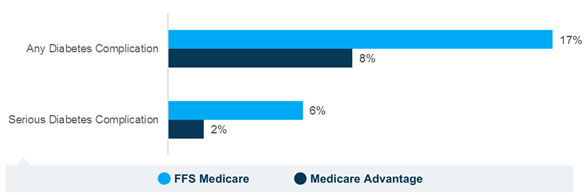
Beyond reaffirming MA’s health and cost-saving prowess compared to FFS models, the study looked at high-need beneficiaries, where MA’s benefits applied as well. MA beneficiaries in a high-need cohort who had clinically complex diabetes had significantly lower rates of complications — serious or otherwise — from diabetes.
Dan Mendelson, president of Avalere, told Healthcare Dive this part of the study is particularly notable. “What’s most compelling here is how capably the plans are addressing serious chronic illness among this population,” Mendelson said. “[MA] plans actually have a higher proportion of individuals with clinical and social risk factors relative to FFS. And that’s significant because that defies a lot of the conventional thinking about who’s going into MA.”
MA’s success — especially in chronic care and high-need populations — reflects the industry-wide push toward value-based care and could energize Congress to further expand the program.
And the program's enrollment continues to grow. MA expanded 8% in 2017 and now accounts for roughly one-third of all Medicare patients, as opposed to 25% six years ago.
CMS announced recently that MA membership will grow an additional 9% to 20.4 million members in 2018. Looking forward, the Congressional Budget Office and HHS both forecast that MA enrollment will continue to grow over the next decade or so, with CBO projecting that about 41% of Medicare beneficiaries will have an MA plan by 2027.
MA is projected to grow in scale, but also in breadth. CMS, aiming to improve quality and affordability, is planning to expand the number of plans available from about 2,700 to more than 3,100 for contract year 2019.
The program is not without critics. Some say it is a slippery slope toward privatization of Medicare, and others note it is not as efficient as proponents claim.
In a shift to addressing social determinants of health, CMS issued a final rule in May granting MA plans more flexibility in supplemental benefit offerings, allowing MA plans to be more adroitly tailored to individual health needs.
“I think MA will continue to grow,” Mendelson agreed, noting that the program's progress has previously been curtailed by the government. “I do think that Congress could help Medicare Advantage grow more rapidly if Congress made it possible for plans to operate in rural and underserved areas. And that, to me, is the next thing that government has to do. Here you see that the plans do well in managing these seriously complex populations and a rational response, from my standpoint, would be to facilitate their growth in rural and underserved areas.”






